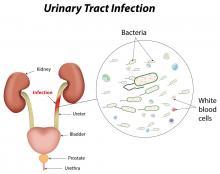
Urinary tract infections (UTIs) can occur in any part of the urinary tract. Most UTIs are caused by bacteria. They can also be caused by fungi or viruses.
UTIs are the second most common type of infection in humans. The National Kidney & Urologic Diseases Information Clearinghouse (NKUDIC) reports that UTIs account for over eight million doctor visits annually.
Antibiotics are used to treat UTIs. Lower UTIs can be treated with oral antibiotics. Upper UTIs require intravenous antibiotics. Sometimes, bacteria develop resistance to antibiotics. Urine cultures can help your doctor select an effective antibiotic treatment.
The following antibiotics are used to treat UTIs:
- Beta-lactams, including penicillins and cephalosporins (for example, Amoxicillin, Augmentin, Keflex, Duricef, Ceftin, Lorabid, Rocephin, Cephalexin, Suprax and others).
- Trimethoprim -sulfamethoxazole combination antibiotic (for example, Bactrim DS and Septra).
- Fluoroquinolones (for example, Cipro, Levaquin and Floxacin), these should not be used in pregnancy or in the pediatric population.
- Tetracyclines (for example, Tetracycline, Doxycycline or Minocycline) used most often for Mycoplasma or Chlamydia infections; like fluoroquinolones, they should not be used in pregnancy or by the pediatric population.
- Aminoglycosides (for example, Gentamycin, Amikacin and Tobramycin used usually in combination with other antibiotics to combat severe UTIs.
- Macrolides (for example, Clarithromycin, Azithromycin and Erythromycin), used more often with some STD (Sexually transmitted diseases like AIDS, Syphilis etc)-caused urinary problems.
There are other antibiotics that are used occasionally, such as Nitrofurantoin, but its use is limited to cystitis and should not be used to treat more serious (kidney) UTIs.
Choice of antibiotics for treatment depends mainly on the susceptibility of the infecting agent to the drug, the seriousness of the infection, if the infected person is an adult, child or is pregnant, and on the treating doctor's experience and knowledge of local antibiotic resistance patterns of commonly infecting bacteria.
Usually, symptoms clear up within a few days of treatment. But you may need to continue antibiotics for a week or more. Take the entire course of antibiotics prescribed by your doctor to ensure that the infection is completely gone.
For an uncomplicated UTI that occurs when you're otherwise healthy, your doctor may recommend a shorter course of treatment, such as taking an antibiotic for one to three days. But whether this short course of treatment is adequate to treat your infection depends on your particular symptoms and medical history. Your doctor may also prescribe a pain medication (analgesic) that numbs your bladder and urethra to relieve burning while urinating. One common side effect of urinary tract analgesics is discolored urine — orange or red.
Frequent infections
If the patient experiences frequent UTIs, the doctor may make certain treatment recommendations, such as:
- Longer course of antibiotic treatment or a programme with short courses of antibiotics at the start of urinary symptoms.
- Home urine tests, in which patient dip a test stick into a urine sample, to check for infection.
- A single dose of antibiotic after sexual intercourse if infections are related to sexual activity.
- Vaginal estrogen therapy if patient is postmenopausal, to minimize chance of recurrent UTIs.
Severe infection
For a severe UTI, patient may need treatment with intravenous antibiotics in a hospital.
Prognosis
A good prognosis is usual for spontaneously resolved and quickly treated UTIs. Even patients who have rapidly developing symptoms and early pyelonephritis can have a good prognosis if quickly and adequately treated. The prognosis begins to decline if the UTI is not quickly recognised or treated.
Elderly and immunosuppressed patients may not have the UTI recognised early; their prognosis may range from fair to poor, depending on how much damage is done to the urinary tract or if complications like sepsis occur. Like adults, most adequately treated children will have a good prognosis. Children and adults with recurrent UTIs may develop complications and a worse prognosis; recurrent UTIs may be a symptom of an underlying problem with the urinary tract structure. These patients should be referred to a specialist (urologist) for further evaluation.
Changed
11/Jan/2016
Condition