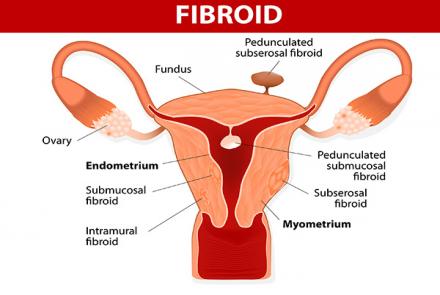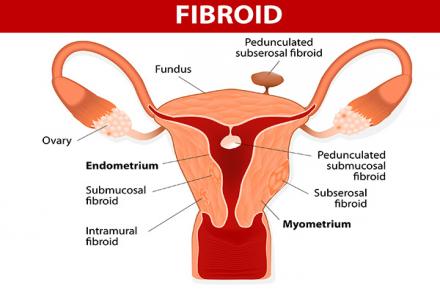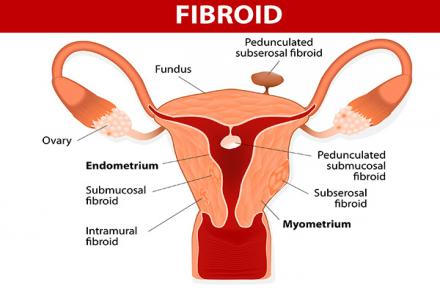
Depending on the location and type of fibroids, the sympoms may vary.
Submucosal: cause heavfibroiy bleeding, long periods and irregular bleeding between the cycles.
Subserosal: cause bulk symptoms, such as pain and pressure in the pelvis, abnormal and excessive menstrual bleeding, pressure on spinal cord.
Intramural: put pressure on the spinal cord, rectum and pelvis, but are asymptomatic unless they grow in size.
Pedunculated: puts pressure on the spinal cord, thus causing lower…

Fibroids are a common occurrence in women between 30 to 50 years of age and are mostly benign, but should be treated keeping in mind the symptoms present and the advice of the treating gynaecologist. Dr. Chandan Dubey, Obstetrician and Gynaecologist answers some of the common questions.
What are fibroids and why do they occur?
Fibroids are benign (not cancer) growths arising from the muscle cells of the uterus. They can range from very small (less than a centimetre) to very large in size. They can remain the same in size, grow slowly or rapidly. The exact cause for fibroids is not known but they are dependent on ovarian hormones - estrogen and progesterone for their growth.
Who is likely to have them?
They are very common and 1 in 4 women are likely to have them though many will be without symptoms. They are more likely to occur in women between 30 to 50 years of age but can occur earlier too. They usually start shrinking in menopause when estrogen levels start decreasing.
What are the symptoms a woman with fibroids is likely to have?
Fibroids may be asymptomatic or cause symptoms like:
- Heavy periods which may last longer and may be painful.
- Irregular bleeding in between periods
- Anemia and associated weakness, tiredness or lethargy.
- Pressure symptoms like increased frequency of passing urine or incomplete bladder emptying if fibroid is pressing on the bladder.
- Fullness, heaviness or bloating of abdomen if very large in size.
- Miscarriage sometimes, if distorting the uterine cavity, or rarely, difficulty in conceiving.
What complications can occur in fibroids?
The fibroids can outgrow their blood supply and undergo degeneration and this can cause pain especially in pregnancy when they grow rapidly sometimes due to the hormonal effects. A fibroid with a long stem may twist on itself and become painful. Fibroids are almost always benign but can become cancerous, even though in rare cases.
How can one find out whether one has fibroids?
Any or a combination of above symptoms would require a visit to a gynecologist who will do a pelvic examination and if necessary a pelvic ultrasound to confirm the clinical findings which may reveal fibroids. Sometimes additional imaging like MRI may be requested.
How would one differentiate between fibroid, endometrios and PMS?
Fibroids and endometriosis can have pelvic pain as a common feature. Adenomyosis is a special kind of uterine endometriosis and may cause heavy periods like fibroids. Sometimes focal adenomyosis can be difficult to differentiate from fibroids even on ultrasound and may need an MRI to clearly distinguish between the two. Ultimately it rests on the gynecologist to make the diagnosis based on a combination of clinical symptoms, signs and imaging studies. Even very severe endometriosis may not be easily diagnosed without an actual visual diagnosis and biopsy on laparoscopy.
PMS is a separate issue altogether and is mostly based on multiple symptoms.
What are the different treatment options for fibroids?
Asymptomatic fibroids may be accidentally discovered in many women and usually do not require any treatment unless very large in size. Fibroids which are symptomatic can be managed in many ways depending on the age of the woman, severity of symptoms, size and location of fibroids and desire for future fertility.
Medical management:
Tranexamic acid, mefenamic acid may sometimes work in reducing mild to moderate heavy periods. Other options like combined oral pills may reduce the heavy flow but not always. Mirena, a progesterone IUD may also help in relieving symptoms of fibroids which are not distorting the cavity of uterus. Some medicines like GnRH hormone injections or ulipristal acetate may be given for upto 3 months before a planned surgical treatment to shrink the fibroids.
Surgical Management:
Myomectomy : this involves surgical removal of the fibroid only and leaving the uterus intact. This is the surgery of choice for women desiring to preserve fertility. The risk of fibroid recurrence is a possibility. In rare cases, a hysterectomy (uterus removal) may have to be done if there is uncontrollable bleeding at the time of myomectomy. Myomectomy may be done by keyhole (laparoscopic) surgery, open surgery or vaginally (hysteroscopically) for fibroids inside the uterine cavity.
Hysterectomy :This is the removal of the uterus surgically and is often used to treat fibroids in women who have completed their family. This surgery can be done via keyhole, open or vaginal routes.
Uterine Artery Embolisation : This is usually done by an interventional radiologist. A catheter is placed in the groin and guided under imaging to reach the major blood vessel supplying the fibroid. Particles are injected to block the vessel and this eventually causes the fibroid to shrink and die. This may not always be successful and some women may require surgery. There are also concerns regarding it's impact on future pregnancies and may not be the best option for women planning to conceive in future.
MR Guided Focussed Ultrasound : Ultrasound beam is focussed on the fibroid with the help of Magnetic resonance imaging (MRI) to destroy the fibroid. This is a relatively newer treatment and its impact on future pregnancy remains to be seen.
How will I know which is the best treatment for me?
The best treatment for a particular patient is to be a joint decision between patient and treating gynaecologist after explaining all procedures, their pros and cons and keeping in mind the patient's expectations, age, symptoms and fertility concerns.
What might be the possible reasons for patients who delay seeking help?
People may delay in seeking help because often the symptoms are mild, and sometimes there may not even be any symptom. In any case, fibroids are mostly benign.
I am eagerly awaiting menopause
What might be the possible impact of not treating fibroids?
The impact of not treating fibroids will depend on the presenting symptoms. Heavy bleeding and anaemia may worsen if not treated.
Changed
10/Feb/2018
Community
Condition